 William Gilbert | William Gilbert, Physician to Queen Elizabeth I, President of the Royal College of Physicians, and creator of the 'magnetic philosophy' introduces the term 'electrica' for objects (insulators) that hold static electricity. He derived the word from the Greek for amber (electra). It was known from ancient times that amber when rubbed could lift light materials. Gilbert added other examples such as sulphur and was describing what would later be known as 'static electricity' to distinguish it from the more noble magnetic force which he saw as part of a philosophy to destroy forever the prevailing Aristotlean view of matter. Gilbert W. De Magnete, magneticisique corporibus, et de magno magnete tellure. 1600 |
 Descarte's reflex ©BIU | The work of Rene Descartes, French Philosopher, is published (after his death) and explains human movement in terms of the complex mechanical interaction of threads, pores, passages and 'animal spirits'. He had worked on his ideas in the 1630s but had abandoned publication because of the persecution of other radical thinkers such as Galileo. William Harvey had developed similar ideas but they were never published. Descartes R. De Homine (Treatise of Man); 1662: Moyardum & leffen, Leiden. |
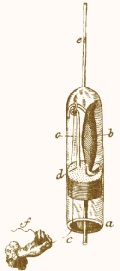 electrical stimulation? ©BIU | Swammerdam refines his experiments on muscle contraction and nerve conduction and demonstrated some to notable figures such as the Grand-Duke Cosimo of Tuscany who was visiting Swammerdam's father's house on the Oude Schans in Amsterdam.
One experiment suspended the muscle on a brass hook inside a glass tube with a water droplet to detect movement and 'irritated' the nerve with a silver wire.
This produced movement of the muscle and it may have been due to the induction of a small electrical charge - although Swammerdam would have been unaware of this.
In the diagram opposite - a) glass tube, b) muscle, c) sliver wire, d) brass wire, e) drop of water, f) investigator's hand. |
 Leyden Jar | Dutch physicist Pieter van Musschenbroek discovers that a partly filled jar with a nail projecting from a cork in its neck can store an electrical charge.
The jar is named the 'Leyden Jar' after the place of its discovery. Ewald Georg von Kliest of Pomerania invented the same device independently.
Using a Leyden jar in 1746, Jean-Antoine Nollet, French physicist and tutor to the Royal family of France sends an electrical current through 180 Royal Guards during a demonstration to King Louis XV. |
A Mr Squires, of Wardour Street, Soho lived opposite the house from which a three year old girl, Catherine Sophia Greenhill had fallen from the first storey window on 16th July 1774. After the attending apothecary had declared that nothing could be done for the child Mr Squires, "with the consent of the parents very humanely tried the effects of electricity. At least twenty minutes had elapsed before he could apply the shock, which he gave to various parts of the body without any apparent success; but at length, upon transmitting a few shocks through the thorax, he perceived a small pulsation: soon after the child began to sigh, and to breathe, though with great difficulty. In about ten minutes she vomited: a kind of stupor, occaisioned by the depression of the cranium, remained for some days, but proper means being used, the child was restored to perfect health and spirits in about a week.
"Mr. Squires gave this astonishing case of recovery to the above gentlemen, from no other motive than a desire of promoting the good of mankind; and hopes for the future that no person will be given up for dead, till various means have been used for their recovery."
Since it is clear she sustained a head injury the electricity probably stimulated the child out of deep coma rather than providing cardiac defibrillation (see also 1788, Charles Kite). Annual Report 1774: Humane Society, London. pp 31-32 Luigi Galvani | Italian Anatomist Luigi Galvani notes that a dissected frog's leg twitches when touched with a metal scalpel.
"I had dissected and prepared a frog in the usual way and while I was attending to something else I laid it on a table on which stood an electrical machine at some distance from its conductor and separated from it by a considerable space. Now when one of the persons present touched accidentally and lightly the inner crural nerves of the frog with the point of a scalpel, all the muscles of the legs seemed to contract again and again as if they were affected by powerful cramps." He later showed that direct contact with the electrical generator or the ground through an electrical conductor would lead to a muscle contraction. Galvani also used brass hooks that attached to the frog's spinal cord and were suspended from an iron railing in a part of his garden. He noticed that the frogs' legs twitched during lightening storms and also when the weather was fine. He interperated these results in terms of "animal electricity" or the preservation in the animal of "nerveo-electrical fluid" similar to that of an electric eel. Galvani's name is given to the 'galvanometer' which is an instrument for measuring (and recording) electricity - this is essentially what an ECG is; a sensitive galvanometer. |
 Alessandro Volta | Alessandro Volta, Italian Scientist and inventor, attempts to disprove Galvani's theory of "animal electricity'" by showing that the electrical current is generated by the combination of two dissimilar metals. His assertion was that the electrical current came from the metals and not the animal tissues. (We now know that both Galvani and Volta were right.) To prove his theory he develops the voltaic pile in 1800 (a column of alternating metal discs - zinc with copper or silver - separated by paperboard soaked in saline) which can deliver a substantial and steady current of electricity. Enthusiasm in the use of electricity leads to further attempts at reanimation of the dead with experiments on recently hanged criminals. Mary Shelly's Frankenstein was published in 1818. Louis Figuier, Les merveilles de la Science (Paris, 1867), p.653 |